
Abdominal aorta
| Abdominal aorta | |
|---|---|
common iliac, Ovarian artery, Median sacral artery | |
| Vein | Inferior vena cava |
| Identifiers | |
| Latin | aorta abdominalis, pars abdominalis aortae |
| MeSH | D001012 |
| TA98 | A12.2.12.001 |
| TA2 | 4205 |
| FMA | 3789 |
| Anatomical terminology] | |
In
Structure
The abdominal aorta begins at the level of the diaphragm, crossing it via the aortic hiatus, technically behind the diaphragm, at the vertebral level of T12.[1] It travels down the posterior wall of the abdomen, anterior to the vertebral column. It thus follows the curvature of the lumbar vertebrae, that is, convex anteriorly. The peak of this convexity is at the level of the third lumbar vertebra (L3). It runs parallel to the inferior vena cava, which is located just to the right of the abdominal aorta, and becomes smaller in diameter as it gives off branches. This is thought to be due to the large size of its principal branches. At the 11th rib, the diameter is 122mm long and 55mm wide and this is because of the constant pressure.[2] The abdominal aorta is clinically divided into 2 segments:
- The suprarenal abdominal or paravisceral segment, diaphragmbut superior to the renal arteries.
- The Infrarenal segment, inferior to the renal arteries and superior to the iliac bifurcation.
Branches
The abdominal aorta supplies blood to much of the abdominal cavity. It begins at T12 and ends at L4 with its bifurcation into the common iliac arteries[1] and usually has the following branches:
| Artery Branch | Vertebra | Type | Paired? | A/P | Description |
inferior phrenic |
T12 | Parietal | yes | post. | Originates above the celiac trunk, below the diaphragm. Passes upward and medially to the suprarenal gland, and crosses crus of diaphragm of corresponding side. Supplies diaphragm and gives superior suprarenal arteries. |
celiac |
T12 | Visceral | no | ant. | Large anterior branch |
| superior mesenteric | L1 | Visceral | no | ant. | Large anterior branch, arises just below celiac trunk |
middle suprarenal |
L1 | Visceral | yes | post. | Crosses crus of diaphragm laterally on each side; supplies the suprarenal gland. |
| renal | In between L1 and L2 | Visceral | yes | post. | Arises just below the superior mesenteric artery. Right renal artery passes deep to the inferior vena cava to right kidney; here it divides into branches. Left renal artery passes deep to the left renal vein. Divides in hilum of kidney. Both arteries give inferior suprarenal arteries and ureteral branches. |
| gonadal | L2 | Visceral | yes | ant. | Ovarian artery in females; testicular artery in males |
| lumbar | L1-L4 | Parietal | yes | post. | Four on each side that supply the abdominal wall and spinal cord. The fifth pair is the lumbar branches of the iliolumbar arteries. They pass deep to the crura on side of vertebral bodies and pass deep to the psoas major and quadratus lumborum to enter the space between the internal oblique and transversus abdominis muscles. Each artery gives off a small dorsal branch, which gives a spinal branch to the vertebral canal and then continues to supply the muscles of the back. |
| inferior mesenteric | L3 | Visceral | no | ant. | Large anterior branch |
| median sacral | L4 | Parietal | no | post. | Artery arising from the middle of the aorta at its lowest part. Represents the continuation of the primitive dorsal aorta; quite large in animals with tails but smaller in humans. |
| common iliac | L4 | Terminal | yes | post. | Branches (bifurcations) to supply blood to the lower limbs and the pelvis, ending the abdominal aorta
|
The bifurcation (union) of the inferior vena cava is at L5 and therefore below that of the bifurcation of the aorta.
.gif)
- inferior phrenic a.
- celiac a.
- left gastric a.
- splenic a.
- short gastric arteries (6)
- splenic arteries (6)
- left gastroepiploic a.
- pancreatic arteries
- common hepatic a.
- right gastric a.
- gastroduodenal a.
- right gastroepiploic a.
- superior pancreaticoduodenal a.
- right hepatic a.
- cystic a.
- left hepatic a.
- superior mesenteric a.
- inferior pancreaticoduodenal a.
- jejunal and ileal arteries
- middle colic a.
- right colic a.
- ileocolic a
- anterior cecal a.
- posterior cecal a. – appendicular a.
- ileal a.
- colic a.
- middle suprarenal a.
- renal a.
- testicular or ovarian a.
- four lumbar arteries
- inferior mesenteric a.
- left colic a.
- sigmoid arteries (2 or 3)
- superior rectal a.
- median sacral a.
- common iliac a.
- external iliac a.
- internal iliac a.
Relations
The abdominal aorta lies slightly to the left of the midline of the body. It is covered, anteriorly, by the
Posteriorly, it is separated from the lumbar vertebrae and intervertebral fibrocartilages by the anterior longitudinal ligament and left lumbar veins.
On the right side it is in relation above with the
On the left side are the left crus of the diaphragm, the left celiac ganglion, the ascending part of the duodenum, and some coils of the small intestine.

Relationship with inferior vena cava
The abdominal aorta's venous counterpart, the inferior vena cava (IVC), travels parallel to it on its right side.
- Above the level of the left renal vein, crossing in front of the aorta.
- Below the level of the umbilicus, the situation is generally reversed, with the aorta sending its right common iliac artery to cross its opposite side counterpart (the left common iliac vein) anteriorly.
Collateral circulation
The collateral circulation would be carried on by the anastomoses between the internal thoracic artery and the inferior epigastric artery; by the free communication between the superior and inferior mesenterics, if the ligature were placed between these vessels; or by the anastomosis between the inferior mesenteric artery and the internal pudendal artery, when (as is more common) the point of ligature is below the origin of the inferior mesenteric artery; and possibly by the anastomoses of the lumbar arteries with the branches of the internal iliac artery.
Clinical significance
Aneurysm
Additional images
-
 Contrast enhanced MRA of the abdominal aorta demonstrating normal paired arteries.
Contrast enhanced MRA of the abdominal aorta demonstrating normal paired arteries. -
 The celiac artery and its branches; the stomach has been raised and the peritoneum removed.
The celiac artery and its branches; the stomach has been raised and the peritoneum removed. -
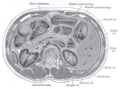 Transverse section through the middle of the first lumbar vertebra, showing the relations of the pancreas.
Transverse section through the middle of the first lumbar vertebra, showing the relations of the pancreas. -
 CT scan showing the liver and a kidney
CT scan showing the liver and a kidney -
 A transverse contrast enhanced CT scan demonstrating an abdominal aortic aneurysm of 4.8 by 3.8 cm
A transverse contrast enhanced CT scan demonstrating an abdominal aortic aneurysm of 4.8 by 3.8 cm -
![The standard aortic measurement on abdominal ultrasonography, such as used for abdominal aortic aneurysms, is between the outer margins of the aortic wall.[3]](//upload.wikimedia.org/wikipedia/commons/thumb/7/7b/Ultrasonographic_measurement_of_aortic_diameter_at_the_navel.svg/120px-Ultrasonographic_measurement_of_aortic_diameter_at_the_navel.svg.png) The standard aortic measurement on abdominal ultrasonography, such as used for abdominal aortic aneurysms, is between the outer margins of the aortic wall.[3]
The standard aortic measurement on abdominal ultrasonography, such as used for abdominal aortic aneurysms, is between the outer margins of the aortic wall.[3] -
 Abdominal aorta
Abdominal aorta -
 Abdominal aorta ultrasound
Abdominal aorta ultrasound





![The standard aortic measurement on abdominal ultrasonography, such as used for abdominal aortic aneurysms, is between the outer margins of the aortic wall.[3]](/File:Ultrasonographic_measurement_of_aortic_diameter_at_the_navel.svg)


See also
- Cardiovascular system
- Nutcracker syndrome
- Aortocaval compression syndrome
References
- ^ a b c
Lech, Christie; Swaminathan, Anand (November 2017). "Abdominal aortic emergencies". Emergency Medicine Clinics of North America. 35 (4): 847–867. PMID 28987432.
- ^ Jim, Jeffrey; Thompson, Robert W. "Clinical features and diagnosis of abdominal aortic aneurysm". UpToDate.
- ^ Jang, Timothy (28 August 2017). "Bedside ultrasonography evaluation of abdominal aortic aneurysm—technique". Medscape.