
Alveolar process
| Alveolar process | |
|---|---|
 Human jaws with anterior (frontal) portion of alveolar processes cut away towards right | |
| Details | |
| Identifiers | |
| Latin | os alveolaris |
| TA98 | A02.1.12.035 |
| TA2 | 791 |
| FMA | 59487 52897, 59487 |
| Anatomical terms of bone | |
The alveolar process (
The synonymous terms alveolar ridge[3] and alveolar margin are also sometimes used more specifically to refer to the ridges on the inside of the mouth which can be felt with the tongue, either on roof of the mouth between the upper teeth and the hard palate or on the bottom of the mouth behind the lower teeth.[4]
Terminology
The term alveolar (
The connected, supporting area of the jaw (delineated by the apexes of the roots of the teeth) is known as the basal bone.[10]
Structure
On the
The alveolar process proper encases the tooth sockets, and contains a lining of
Although the alveolar process is composed of compact bone, it may be called the cribriform plate because it contains numerous holes where Volkmann's canals pass from the alveolar bone into the PDL. The alveolar bone proper is also called bundle bone because Sharpey's fibres, part of the PDL, are inserted there. Sharpey's fibres in alveolar bone proper are inserted at a right angle (just as with the cemental surface); they are fewer in number, but thicker in diameter than those found in cementum.[8]The supporting alveolar bone consists of both cortical (compact) bone and
The alveolar structure is a dynamic tissue which provides the jawbone with some degree of flexibility and resilience for the embedded teeth as they encounter numerous multi-directional forces.[15][16]
Composition
Alveolar bone is 67% inorganic material, composed mainly of the minerals
The cellular component of bone consists of osteoblasts, osteocytes and osteoclasts.[17]
Clinical significance
Alveolar bone loss
Bone is lost through the process of resorption which involves osteoclasts breaking down the hard tissue of bone. A key indication of resorption is when scalloped erosion occurs. This is also known as Howship's lacuna.[18] The resorption phase lasts as long as the lifespan of the osteoclast which is around 8 to 10 days. After this resorption phase, the osteoclast can continue resorbing surfaces in another cycle or carry out apoptosis. A repair phase follows the resorption phase which lasts over 3 months. In patients with periodontal disease, inflammation lasts longer and during the repair phase, resorption may override any bone formation. This results in a net loss of alveolar bone.[19]
Alveolar bone loss is closely associated with periodontal disease. Periodontal disease is the inflammation of the gums. Studies in osteoimmunology have proposed 2 models for alveolar bone loss. One model states that inflammation is triggered by a periodontal pathogen which activates the acquired immune system to inhibit bone coupling by limiting new bone formation after resorption.[20] Another model states that cytokinesis may inhibit the differentiation of osteoblasts from their precursors, therefore limiting bone formation. This results in a net loss of alveolar bone.[21]
Developmental disturbances
The developmental disturbance of anodontia (or hypodontia, if only one tooth), in which tooth germs are congenitally absent, may affect the development of the alveolar processes. This occurrence can prevent the alveolar processes of either the maxillae or the mandible from developing. Proper development is impossible because the alveolar unit of each dental arch must form in response to the tooth germs in the area.[22]
Pathology
After extraction of a tooth, the clot in the alveolus fills in with immature bone, which later is remodeled into mature secondary bone. Disturbance of the blood clot can cause alveolar osteitis, commonly referred to as "dry socket". With the partial or total loss of teeth, the alveolar process undergoes resorption. The underlying basal bone of the body of the maxilla or mandible remains less affected, however, because it does not need the presence of teeth to remain viable. The loss of alveolar bone, coupled with attrition of the teeth, causes a loss of height of the lower third of the vertical dimension of the face when the teeth are in maximum intercuspation. The extent of this loss is determined based on clinical judgment using the Golden Proportions.[22]
The density of the alveolar bone in a given area also determines the route that dental infection takes with abscess formation, as well as the efficacy of local infiltration during the use of local anesthesia. In addition, the differences in alveolar process density determine the easiest and most convenient areas of bony fracture to be used, if needed during tooth extraction of impacted teeth.[22]
During chronic
The radiographic integrity of the lamina dura is important in detecting pathological
Alveolar bone grafting

Alveolar bone grafting in the mixed dentition is an essential part of the reconstructive journey for cleft lip and cleft palate patients. The reconstruction of the alveolar cleft can provide both aesthetic and practical advantages to the patient.[23] Alveolar bone grafting can also bring about the following benefits: stabilisation of the maxillary arch; aid of eruption of the canine and sometimes lateral incisor eruption; offering bony support to the teeth lying next to the cleft; elevate the alar base of the nose; aid sealing of oro-nasal fistula; permit insertion of a titanium fixture in the grafted region and achieve good periodontal conditions within and next to the cleft.[24] The timing of the alveolar bone grafting takes into consideration both eruption of the canine and lateral incisor. The optimal time for bone grafting surgery is when a thin shell of bone still covers the soon erupting lateral incisor or canine tooth close to the cleft.[24]
- Primary bone grafting: Primary bone grafting is believed to: eliminate bone deficiency, stabilize pre-maxilla, synthesize new bone matrix for eruption of teeth in the cleft area and augment the alar base. However, the early bone grafting procedure is abandoned in most cleft lip and palate centres around the world due to many disadvantages, including serious growth disturbances of the middle third of the facial skeleton. The operative technique that involves the vomero-premaxillary suture was found to inhibit maxillary growth.[24]
- Secondary bone grafting: Secondary bone grafting, also referred to as bone grafting in the mixed dentition, became a well-established procedure after abandoning primary bone grafting. The prerequisites include precise timing, operating technique, and acceptably vascularized soft tissue. The advantages of primary bone grafting, which are allowing tooth eruption through the grafted bone, are retained. Furthermore, secondary bone grafting stabilizes the maxillary arch, thus enhancing the conditions for prosthodontic treatment such as crowns, bridges and implants. It also aids eruption of teeth, boosting the amount of bony tissue on the alveolar crest, permitting orthodontic treatment. Bony support to teeth adjacent to the cleft is a pre-requisite for orthodontic closure of the teeth in the cleft region. Hence, better hygienic conditions will be achieved which helps to lessen formation of caries and periodontal inflammation. Speech problems caused by irregular positioning of articulators, or leakage of air via the oronasal communication, may also be improved. Secondary bone grafting can also be used to augment the alar base of the nose to achieve symmetry with the non-cleft side, thereby enhancing facial appearance.[24]
- Late secondary bone grafting: Bone grafting has a lower success rate when performed after canine has erupted as compared to before the eruption. It has been found that the possibility for orthodontic closure of the cleft in the dental arch is smaller in patients grafted before canine eruption than those after the canine eruption. The surgical procedure includes drilling of several small openings through the cortical layer into the cancellous layer, facilitating growth of blood vessels into the graft.[24]
Congenital epulis
Diagnosis of the condition was previously incidental, however, with improvements in imaging technology, prenatal diagnosis is now possible at 26 weeks (about 6 months). Furthermore, these benign lesions can be treated by surgical excision.[25]
Dentistry
The alveolar ridge is an area of particular interest in dentistry, as preservation of the ridges results in a higher success rate of therapeutic dental treatments.[27]
Grafting materials
Grafting is an effective technique to reduce the inevitable changes in dimension of the alveolar ridge after tooth extraction.[28] The type of grafting material is important as different materials are more effective than others in maintaining the alveolar ridge.[29]
No biomaterial can prevent alveolar bone loss entirely after extraction, however, there are five grafting materials with the greatest efficacy in height resorption prevention; three of which are
For the best outcomes with respect to horizontal alveolar ridge preservation, application of a xenogenic (non-living bone material from another species) or allogenic grafting material (bone donated by another human) surrounded by a resorbable collagen membrane or sponge is ideal.
Dental implants
.jpg)
The alveolar ridge refers to one of the two thickened bony crests, that exists in the upper and lower portions of the jawbone and house the sockets of the teeth.
Articulation
]).Culture
Other than a maxillar bridge made of gold, part of a mandible with teeth—which had been burned and broken around the alveolar process—was the only physical evidence used to confirm Adolf Hitler's death in 1945.[42][43][44] According to Eva Braun's purported Soviet autopsy report, the alveolar process was missing from her charred maxilla.[45]
Gallery
-
 Superior area of the alveolar process on the mandible
Superior area of the alveolar process on the mandible -
 The alveolar process of the maxilla is located at its inferior surface.
The alveolar process of the maxilla is located at its inferior surface. -
 3D animation showing placement of teeth in human skull
3D animation showing placement of teeth in human skull -
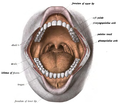 In the oral cavity, the alveolar processes are covered by gums.
In the oral cavity, the alveolar processes are covered by gums. -
 How the roots of the teeth, gums, and alveolar bone are related
How the roots of the teeth, gums, and alveolar bone are related -
 Eroded alveolar process of the archaic human Homo heidelbergensis
Eroded alveolar process of the archaic human Homo heidelbergensis






References
- ISBN 9781405881180.
- ^ a b Bath-Balogh & Fehrenbach 1997, p. 195.
- ^ "Definition of ALVEOLAR PROCESS". www.merriam-webster.com. Retrieved 9 March 2022.
- ^ Phonetics at the Encyclopædia Britannica Accessed: 12 September 2018.
- ^ "alveolar | Origin and meaning of alveolar". Online Etymology Dictionary. Retrieved 31 August 2021.
- PMID 30958300.
- ^ Araujo M, Lindhe J (2003). "The Edentulous Alveolar Ridge.". In Lindhe J, Karring T, Lang NP (eds.). Clinical Periodontology and Implant Dentistry (5th ed.). Oxford: Blackwell Munksgaard. pp. 53–63.
- ^ a b c d e f Bath-Balogh & Fehrenbach 1997, p. 196.
- ^ Bath-Balogh & Fehrenbach 1997, pp. 199–200.
- ^ Bath-Balogh & Fehrenbach 1997, pp. 195–197.
- PMID 21250078, retrieved 30 August 2021
- ^ Bath-Balogh & Fehrenbach 1997, pp. 196, 198.
- ^ a b Ten Cate's Oral Histology, Nanci, Elsevier, 2013, page 219
- ^ Bath-Balogh & Fehrenbach 1997, pp. 198–99.
- PMID 26177631.
- S2CID 27295301.
- ^ OCLC 971599883.
- S2CID 21096888.
- OCLC 51892824.
- PMID 16552059.
- PMID 21135192.
- ^ a b c Bath-Balogh & Fehrenbach 1997.
- PMID 24179451.
- ^ PMID 19884665.Material was copied from this source, which is available under a Creative Commons License.

- ^ ISSN 2638-4809.
- ^ PMID 34189098.
- PMID 26132885.
- ^ PMID 24966231.
- ^ S2CID 235659457.
- PMID 31069040.
- S2CID 58649044.
- PMID 32050433.
- PMID 27878769.
- ^ PMID 27563613.
- PMID 31932579.
- PMID 28979109.
- PMID 31077190.
- ^ PMID 32606277.
- PMID 30341270.
- PMID 30306698.
- PMID 27008252.
- ISBN 978-1-85409-465-0.
- Harcourt, Brace & World. p. 45.
- S2CID 29159362.
- Harcourt, Brace & World. p. 111.
Sources
- Bath-Balogh, Mary; Fehrenbach, Margaret J. (1997). Illustrated Dental Embryology, Histology, and Anatomy. ISBN 0-7216-6687-6.
External links
- Photo of model at Waynesburg College skeleton/alveolarprocess
- "Anatomy diagram: 34256.000-1". Roche Lexicon – illustrated navigator. Elsevier. Archived from the original on 27 December 2012.
- Diagram at case.edu
{kind=link}