
Avascular necrosis
| Avascular necrosis | |
|---|---|
| Other names | Osteonecrosis, Legg–Calvé–Perthes syndrome, sickle cell disease[3] |
| Treatment | Medication, not walking on the affected leg, stretching, surgery[1] |
| Frequency | ~15,000 per year (US)[4] |
Avascular necrosis (AVN), also called osteonecrosis or bone infarction, is
Risk factors include
Treatments may include medication, not walking on the affected leg, stretching, and surgery.
About 15,000 cases occur per year in the United States.[4] People 30 to 50 years old are most commonly affected.[3] Males are more commonly affected than females.[4]
Signs and symptoms
In many cases, there is pain and discomfort in a joint which increases over time. It can affect any bone, and for in about half of affected people, multiple sites are damaged.[5]
Avascular necrosis most commonly affects the ends of long bones, such as the femur. Other common sites include the humerus (upper arm),[6][7] knees,[8][9] shoulders,[6][7] ankles and the jaw.[10]
Causes
The main risk factors are
Prolonged, repeated exposure to high pressures (as experienced by commercial and military divers) has been linked to AVN, though the relationship is not well understood.[14][15]
In children, avascular osteonecrosis can have several causes. It can occur in the hip as part of
Pathophysiology
The
Upon
Diagnosis
In the early stages,
X-ray images of avascular necrosis in the early stages usually appear normal. In later stages it appears relatively more radio-opaque due to the nearby living bone becoming
-
 Radiography of total avascular necrosis of right humeral head. Woman of 81 years with diabetes of long evolution.
Radiography of total avascular necrosis of right humeral head. Woman of 81 years with diabetes of long evolution. -
 Radiography of avascular necrosis of left femoral head. Man of 45 years withAIDS.
Radiography of avascular necrosis of left femoral head. Man of 45 years withAIDS. -
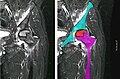 Nuclear magnetic resonance of avascular necrosis of left femoral head. Man of 45 years with AIDS.
Nuclear magnetic resonance of avascular necrosis of left femoral head. Man of 45 years with AIDS. -
![The intravertebral vacuum cleft sign (at white arrow) is a sign of avascular necrosis. Avascular necrosis of a vertebral body after a vertebral compression fracture is called Kümmel's disease.[20]](//upload.wikimedia.org/wikipedia/commons/thumb/6/66/Intravertebral_vacuum_cleft_sign.jpg/120px-Intravertebral_vacuum_cleft_sign.jpg) The intravertebral vacuum cleft sign (at white arrow) is a sign of avascular necrosis. Avascular necrosis of a vertebral body after a vertebral compression fracture is called Kümmel's disease.[20]
The intravertebral vacuum cleft sign (at white arrow) is a sign of avascular necrosis. Avascular necrosis of a vertebral body after a vertebral compression fracture is called Kümmel's disease.[20] -
 Pathology of avascular necrosis, with a photograph of a cross-section of the involved bone at top left. The reactive zone shows irregular trebaculae with empty lacunae, and fibrosis of the marrow space.
Pathology of avascular necrosis, with a photograph of a cross-section of the involved bone at top left. The reactive zone shows irregular trebaculae with empty lacunae, and fibrosis of the marrow space.



![The intravertebral vacuum cleft sign (at white arrow) is a sign of avascular necrosis. Avascular necrosis of a vertebral body after a vertebral compression fracture is called Kümmel's disease.[20]](/File:Intravertebral_vacuum_cleft_sign.jpg)

Types
When AVN affects the scaphoid bone, it is known as Preiser disease. Another named form of AVN is Köhler disease, which affects the navicular bone of the foot, primarily in children. Yet another form of AVN is Kienböck's disease, which affects the lunate bone in the wrist.[21]
Treatment
A variety of methods may be used to treat
Other techniques such as metal on metal resurfacing may not be suitable in all cases of avascular necrosis; its suitability depends on how much damage has occurred to the femoral head.
Core decompression
Other treatments include core decompression, where internal bone pressure is relieved by drilling a hole into the bone, and a living bone chip and an electrical device to stimulate new vascular growth are implanted; and the free vascular fibular graft (FVFG), in which a portion of the fibula, along with its blood supply, is removed and transplanted into the femoral head.[25] A 2016 Cochrane review found no clear improvement between people who have had hip core decompression and participate in physical therapy, versus physical therapy alone. There is additionally no strong research on the effectiveness of hip core decompression for people with sickle cell disease.[11]
Progression of the disease could possibly be halted by transplanting nucleated cells from bone marrow into avascular necrosis lesions after core decompression, although much further research is needed to establish this technique.[26][27]
Prognosis
The amount of disability that results from avascular necrosis depends on what part of the bone is affected, how large an area is involved, and how effectively the bone rebuilds itself. The process of bone rebuilding takes place after an injury as well as during normal growth.[23] Normally, bone continuously breaks down and rebuilds—old bone is resorbed and replaced with new bone. The process keeps the skeleton strong and helps it to maintain a balance of minerals.[23] In the course of avascular necrosis, however, the healing process is usually ineffective and the bone tissues break down faster than the body can repair them. If left untreated, the disease progresses, the bone collapses,[28] and the joint surface breaks down, leading to pain and arthritis.[1]
Epidemiology
Avascular necrosis usually affects people between 30 and 50 years of age; about 10,000 to 20,000 people develop avascular necrosis of the head of the femur in the US each year.[citation needed]
Society and culture
Cases of avascular necrosis have been identified in a few high-profile athletes. It abruptly ended the career of
Another high-profile athlete was American
See also
- Sperm whale skeletons can show damage from avascular necrosis caused by decompression.[35]
References
- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z "Questions and Answers about Osteonecrosis (Avascular Necrosis)". NIAMS. October 2015. Archived from the original on 9 August 2017.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain.
- ^ a b c d e f g h Khan AN, Al-Salman MJ, Chandramohan M, MacDonald S, Hutchinson CE. "Bone Infarct". eMedicine Specialties. Archived from the original on 4 March 2010.
- ^ a b "Osteonecrosis". NORD (National Organization for Rare Disorders). 2009. Archived from the original on 19 February 2017. Retrieved 8 August 2017.
- ^ ISBN 9780323529570. Archivedfrom the original on 9 August 2017.
- ^ Food and Drug Administration. Archivedfrom the original on 23 May 2009. Retrieved 25 May 2009.
- ^ PMID 15525936.
- ^ PMID 15789002.
- S2CID 16423679. Archived from the original(PDF) on 26 July 2020.
- S2CID 3235011.
- PMID 15547404.
- ^ PMID 31803937.
- ^ Campbell, Ernest S. (4 April 2019). "Dysbaric Osteonecrosis and Diving". SCUBADOC - Diving Medicine Online. SCUBADOC. Retrieved 20 April 2021.
- PMID 17236837.
- PMID 25562949.
- S2CID 20119213.
- S2CID 260321190.
- PMID 21512065.
- S2CID 40304352.
- S2CID 2554184.
- S2CID 15539206.
- ISSN 0030-5898.
- ^ PMID 30782340.
- ^ ISBN 978-0-936923-24-6.
- PMID 15572396.
- S2CID 25970488.
- PMID 15743852. Archived from the originalon 14 February 2009. Retrieved 27 April 2010.
- S2CID 25883407.
- S2CID 31296534.
- ^ Altman LK (20 March 1991). "Jackson's Case Is Dividing The Doctors". The New York Times.
- ^ "What, his hip? Favre reveals he has avascular necrosis". JS Online. 27 September 2006. Archived from the original on 27 September 2006.
- ^ "What He's Been Pedaling". The New York Times. 16 July 2006.
- ^ "Landis Tests Positive; Title is a total complete loss". Chicago Tribune. 5 August 2006.
- ^ Fotheringham A (24 July 2006). "Cycling: Landis the Tour king celebrates a triumph of survival". The Independent. London. Archived from the original on 6 August 2006. Retrieved 28 July 2006. (subscription required)
- ^ Roy, Neelabhra (13 May 2022). "What is Mueller-Weiss Syndrome, the foot injury Rafael Nadal suffers from?". www.sportskeeda.com. Retrieved 5 June 2022.
- PMID 15618509.
External links
- Osteonecrosis / Avascular Necrosis at the National Institute of Health
- Osteonecrosis / Avascular necrosis at Merck Manualfor patients
- Osteonecrosis / Avascular necrosis at Merck Manualfor medical professionals