
Coronary circulation
| Coronary circulation | |
|---|---|
 Blood vessels of the coronary circulation of the human heart viewed from the front and from behind | |
| Identifiers | |
| MeSH | D003326 |
| Anatomical terminology | |
Coronary circulation is the
Structure
Coronary arteries


The left coronary artery distributes blood to the left side of the heart, the left atrium and ventricle, and the interventricular septum. The
The right coronary artery proceeds along the coronary sulcus and distributes blood to the right atrium, portions of both ventricles, and the
Cardiac veins

The
Anastomoses
There are some anastomoses between branches of the two coronary arteries. However the coronary arteries are functionally end arteries and so these meetings are referred to as potential
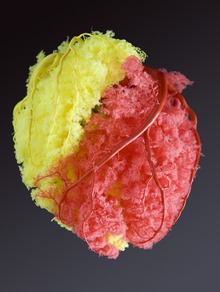
Under the most common configuration of coronary arteries, there are three areas of anastomoses. Small branches of the LAD (left anterior descending/anterior interventricular) branch of the left coronary join with branches of the posterior interventricular branch of the right coronary in the interventricular sulcus (groove). More superiorly, there is an anastomosis between the circumflex artery (a branch of the left coronary artery) and the right coronary artery in the atrioventricular groove. There is also an anastomosis between the septal branches of the two coronary arteries in the interventricular septum. The photograph shows area of heart supplied by the right and the left coronary arteries.[citation needed]
Variation
The left and right coronary arteries occasionally arise by a common trunk, or their number may be increased to three; the additional branch being the posterior coronary artery (which is smaller in size). In rare cases, a person will have the third coronary artery run around the root of the aorta.[citation needed]
Occasionally, a coronary artery will exist as a double structure (i.e. there are two arteries, parallel to each other, where ordinarily there would be one).[citation needed]
Coronary artery dominance
The artery that supplies the posterior third of the interventricular septum – the posterior descending artery (PDA)[3] determines the coronary dominance.[4]
- If the posterior descending artery is supplied by the right coronary artery (RCA), then the coronary circulation can be classified as "right-dominant."
- If the posterior descending artery is supplied by the circumflex artery (CX), a branch of the left artery, then the coronary circulation can be classified as "left-dominant."
- If the posterior descending artery is supplied by both the right coronary artery and the circumflex artery, then the coronary circulation can be classified as "co-dominant."
Approximately 70% of the general population are right-dominant, 20% are co-dominant, and 10% are left-dominant.[4] A precise anatomic definition of dominance would be the artery which gives off supply to the AV node i.e. the AV nodal artery. Most of the time this is the right coronary artery.[citation needed]
Function
Supply to papillary muscles
The
The anterolateral papillary muscle more frequently receives two blood supplies:
Changes in diastole
During contraction of the
Changes in oxygen demand
The heart regulates the amount of vasodilation or vasoconstriction of the coronary arteries based upon the oxygen requirements of the heart. This contributes to the filling difficulties of the coronary arteries. Compression remains the same. Failure of oxygen delivery caused by a decrease in blood flow in front of increased oxygen demand of the heart results in tissue
In addition to metabolism, the coronary circulation possesses unique pharmacologic characteristics. Prominent among these is its reactivity to adrenergic stimulation.[citation needed]
Branches
The following are the named branches of the coronary circulation in a right-dominant heart:[citation needed]
- Aorta
- Left coronary artery / Left main coronary artery (LMCA)
- Left circumflex artery(LCX)
- Obtuse marginal artery#1 (OM1)
- Obtuse marginal artery#2 (OM2)
- Left anterior descending artery (LAD)
- Right coronary artery (RCA)
- Atrioventricular nodal branch
- Right marginal artery
- Posterior descending artery (PDA)
- Posteriolateral artery #1 (PL#1)
- Posteriolateral artery #2 (PL#2)
- Left coronary artery / Left main coronary artery (LMCA)
Clinical significance
The
The relatively narrow coronary arteries are commonly affected by
Additional images
-
 Anterior view of coronary circulation
Anterior view of coronary circulation -
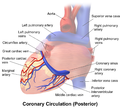 Posterior view of coronary circulation
Posterior view of coronary circulation -
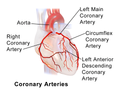 Illustration of coronary arteries
Illustration of coronary arteries



See also
- Anomalous aortic origin of a coronary artery
- Cardiac skeleton
- Coronary sinus
- Coronary steal
- Cardiology
- Left coronary artery
- Right coronary artery
References
This article incorporates text from the
- ^ ISBN 978-1938168130. Retrieved 11 August 2014.
- ^ www.radiopaedia.org/
- ^ 00460 at CHORUS
- ^ ISBN 0-07-135694-0.
- ^ PMID 7882478.
- PMID 19966048. Retrieved 26 May 2021.