
Dopamine antagonist
| Dopamine receptor antagonist Dopaminergic blockers | |
|---|---|
N05A | |
| Biological target | Dopamine receptors |
| External links | |
| MeSH | D012559 |
| Legal status | |
| In Wikidata | |
A dopamine antagonist, also known as an anti-dopaminergic and a dopamine receptor antagonist (DRA), is a type of
.Receptor pharmacology

Dopamine receptors are all
D1-like receptors: D1 and D5
D1-like receptors – D1 and D5 are always found post-synaptically. The genes coding these receptors lack introns, so there are no splice variants.
D1 receptors
- D1 receptors are found mainly on neurons in the nucleus accumbens[3] as well as substantia nigra,[2] striatum,[2] amygdala,[2] frontal cortex[2] and olfactory bulb and retina[2]
- Also found (in lower levels) in the hypothalamus, thalamus, cerebellum and hippocampus[2]
- Peripherally, these receptors have been found in the renal artery, mesenteric artery, and splenic artery where activation leads to vasodilation.[4] In addition, D1 receptors have been found in the kidney[4]
D5 receptors
- Low levels of D5 receptors have been found in the hypothalamus, prefrontal cortex and cingulate cortex; as well as memory areas such as hippocampus, dentate gyrus and entorhinal cortex.[2]
- In addition, D5 receptors have been found in the kidney[4]
D2-like receptors: D2, D3 and D4
D2-like receptors unlike the D1-like class, these receptors are found pre and post-synaptically. The genes that code these receptors have introns, leading to many alternately spliced variants.
D2 receptors
- D2 receptors are found in the striatum, substantia nigra, ventral tegmental area, hypothalamus, cortex, septum, amygdala, hippocampus, and olfactory tubercle.[2]
- These receptors have also been found in the retina and pituitary gland.[2]
- Peripherally, these receptors have been found in the renal, mesenteric, and splenic arteries as well as on the adrenal cortex and medulla and within the kidney.[4]
D3 receptors
- D3 receptors are highly expressed on neurons in islands of Calleja and nucleus accumbens shell and lowly expressed in areas such as the substantia nigra pars compacta, hippocampus, septal area, and ventral tegmental area.[2][3]
- Additional studies have found these receptors peripherally in the kidney[4]
D4 receptors
- D4 receptors are found in amygdala, hippocampus, hypothalamus, globus pallidus, substantia nigra pars reticula, the thalamus, the retina and the kidney[2][4]
Implications in disease
The dopaminergic system has been implicated in a variety of disorders. Parkinson's disease results from loss of dopaminergic neurons in the striatum.[5] Furthermore, most effective antipsychotics block D2 receptors, suggesting a role for dopamine in schizophrenia.[5][6][7] Additional studies hypothesize dopamine dysregulation is involved in Huntington's disease, ADHD, Tourette's syndrome, major depression, manic depression, addiction, hypertension and kidney dysfunction.[5][7][8] Dopamine receptor antagonists are used for some diseases such as schizophrenia, bipolar disorder, nausea and vomiting.[5]
- Melatonin suppresses dopamine activity[9] as part of normal circadian rhythm functions, although pathological imbalances have been implicated in Parkinson's disease[10]
Side effects
They may include one or more of the following and last indefinitely even after cessation of the dopamine antagonist, especially after long-term or high-dosage use:
- Cardiovascular disease[11][12]
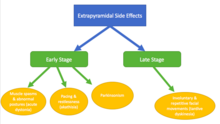
- Extrapyramidal symptoms (EPS) associated with typical antipsychotics:
- Early stage – occurs at onset of treatment or following increased dose, patients recover when dose is decreased[13]
- Acute dystonias[13] – muscle spasms and sustained abnormal postures and onset occurs within a few days; can be treated with anticholinergics
- risk factors include age, gender and family history[13]
- Akathisia[13][14] - pacing and restlessness and onset occurs within the first few months; can be treated with beta blockers and benzodiazepines
- Parkinsonism due to effects on the nigrostriatal pathway[13][14] - includes tremors, bradykinesia and muscle rigidity
- risk factors include age and gender[13]
- Acute dystonias[13] – muscle spasms and sustained abnormal postures and onset occurs within a few days; can be treated with anticholinergics
- Late stage – occurs after prolonged (months-years) treatment, symptoms persist even after dose is decreased[13]
- Tardive dyskinesia[13][14] - includes involuntary and repetitive facial movements
- risk factors include age, race and gender[13]
- Tardive dyskinesia[13][14] - includes involuntary and repetitive facial movements
- It is hypothesized that these effects are due to chronic blockade of the D2 receptor[14]
- Early stage – occurs at onset of treatment or following increased dose, patients recover when dose is decreased[13]
- Hyperprolactinaemia due to blockade of the D2 receptors in the anterior pituitary leading to increased prolactin release[11][15]
- Increased appetite including increased craving and binge eating that lead to weight gain[11][16][17]
- Increased risk for insulin resistance[16]
- Sexual dysfunction[11][12]
- Metabolic changes with increased risk of
- Sedation[11][12]
- Neuroleptic Malignant Syndrome[18] is a medical emergency caused by a decrease in dopaminergic activity, resulting in a central D2 receptor blockade.[18]

Examples
First-generation antipsychotics (typical)
First generation antipsychotics are used to treat schizophrenia and are often accompanied by extrapyramidal side effects.[19] They inhibit dopaminergic neurotransmission in the brain by blocking about 72% of the D2 dopamine receptors.[20] They can also block noradrenergic, cholinergic, and histaminergic activity.[20]
- Benperidol[19] binds D2 and some serotonin receptors.[21] It is absorbed very easily and has a high first pass effect.[21]
- Chlorpromazine binds D3 with the highest affinity, but also binds D1, D2, D4 and D5[22][23]

- Clopenthixol[19]
- Droperidol is used as an antipsychotic and antiemetic.[19]
- Haloperidol binds D2, D3 and D4 with the highest affinity, but also binds D1 and D5.[19][22][23] Haloperidol also has a risk for QTc prolongation. [24]
- Fluphenazine binds D2 and D3 with the highest affinity but D1 and D5 as well[19][22]
- Flupentixol binds D1, D2, D3, and D5[22] and is also used as an antidepressant.[19]
- Fluspirilene[19]
- Penfluridol[19]
- Perazine[19]
- Perphenazine[19]
- Pimozide binds D2 and D3 with high affinity, also binds D4 receptors[19][22]
- Sulpiride binds D2 and D3[19][22] and is also used as an antidepressant.[19]
- Thioridazine binds D2, D3 and D4 with high affinity; can also bind D1 and D5 at higher concentrations[22] Thioridazine has the highest associated risk of QTc prolongation among neuroleptics.[24]
Second-generation antipsychotics (atypical)
These drugs are not only dopamine antagonists at the receptor specified, but also act on serotonin receptor 5HT2A.[20][25] These drugs have fewer extrapyramidal side effects and are less likely to affect prolactin levels when compared to typical antipsychotics.[26]
- Amisulpride binds D2 and D3[27] and is used as an antipsychotic, antidepressant and also treats bipolar disorder.[25] It treats both the positive and negative symptoms of schizophrenia.[28]
- Asenapine binds D2, D3 and D4[29] and is used to treat bipolar disorder and schizophrenia.[30] Its side effects include weight gain but there is lower risk for orthostatic hypotension and hyperprolactinemia.
- Aripiprazole binds D2 as a partial agonist but antagonizes D3.[31] In addition, aripiprazole treats schizophrenia, bipolar disorder (mania),[32] depression,[25] and tic disorders[31]

- Clozapine binds D1 and D4 with the highest affinity but still binds D2 and D3.[33] Clozapine is unique because it is only prescribed when treatment with at least two other antipsychotics has failed due to its very harsh side effects.[34] It also requires weekly white blood cell counts to monitor potential neutropenia.[34]
- Loxapine binds D2, D3 and D4 with high affinity; can also bind D1.[35] Loxapine is often used to treat agitated and violent patients with neuropsychiatric disorders such as bipolar disorder and schizophrenia.[36]
- Nemonapride binds D3, D4 and D5.[37]
- Olanzapine binds all receptors[38] and is used to treat the positive and negative symptoms of schizophrenia as well as bipolar disorder and depression.[39] It has been associated with significant weight gain.[40]
- Quetiapine binds D1, D2 and D3 and can bind D4 at high concentrations.[38] It is used to treat the positive symptoms of schizophrenia,[40] bipolar disorder and depression.[39] Of the second generation antipsychotics, quetiapine may produce fewer parkinsonian side effects.[41]
- Paliperidone binds D2, D3 and D4 with high affinity; can also bind D1 and D5.[42]
- Remoxipride binds D2 receptors with relatively low affinity.[38][43][39]
- Risperidone binds D2, D3 and D4 receptors.[39][38][42] Risperidone not only treats the positive and negative symptoms of schizophrenia[40] but also treats bipolar disorder.[39]
- Tiapride blocks D2 and D3 and is used as an antipsychotic.[39] It is also often used to treat dyskinesias, psychomotor agitations, tics, Huntington's chorea and alcohol dependence.[44]
- Ziprasidone blocks the D2 receptor[45] and is used to treat schizophrenia, depression and bipolar disorder.[39] There is controversy on whether Ziprasidone treats negative symptoms and it has well documented gastrointestinal side effects.[40] Ziprasidone can also cause QTc prolongation.[24]
Dopamine antagonists used to treat nausea and vomiting
- Domperidone is a peripherally selective dopamine D2 receptor antagonist used as an antiemetic, gastroprokinetic agent and galactagogue.
- Bromopride binds enteric D2 receptors[46] and also treats gastroparesis.[47]
- Metoclopramide also treats gastroparesis[47]
Antagonists used only in research settings
- Eticlopride binds D2 and D3 with high affinity but also binds D4[48][49][50]
- Nafadotride binds D2 and D3[47][48][49]
- Raclopride binds D2 and D3[47][48] and can be radiolabeled and used in PET imaging to identify disease progression in Huntington's Disease[51]
References
- S2CID 2545878.
- ^ S2CID 2545878.
- ^ PMID 16613552.
- ^ PMID 9457173.
- ^ S2CID 2545878.
- S2CID 30902536.
- ^ PMID 9457173.
- S2CID 22686973.
- S2CID 25508148.
- S2CID 29375454.
- ^ S2CID 8345032.
- ^ PMID 10811237.
- ^ PMID 24995318.
- ^ PMID 9457173.
- PMID 11607043.
- ^ PMID 24011886.
- PMID 14972081.
- ^ PMID 23983836.
- ^ S2CID 2545878.
- ^ PMID 30137788– via NCBI.
- ^ PMID 15846648.
- ^ PMID 16613552.
- ^ PMID 9457173.
- ^ PMID 23295003.
- ^ S2CID 2545878.
- PMID 11607043.
- PMID 16613552.
- PMID 14972081.
- PMID 22494521.
- PMID 26674884.
- ^ PMID 26220447.
- PMID 24346956.
- PMID 16613552.
- ^ PMID 14972081.
- PMID 25859275.
- S2CID 4402288.
- PMID 9457173.
- ^ PMID 16613552.
- ^ S2CID 2545878.
- ^ PMID 14972081.
- PMID 24249315.
- ^ PMID 25943458.
- PMID 11607043.
- S2CID 260238868.
- PMID 14728084.
- PMID 14871277.
- ^ S2CID 2545878.
- ^ PMID 16613552.
- ^ PMID 9457173.
- PMID 18801115.
- PMID 26899245.
External links
- Dopamine+antagonists at the U.S. National Library of Medicine Medical Subject Headings (MeSH)