
Epidural hematoma
| Epidural hematoma | |
|---|---|
| Other names | Extradural hematoma, epidural hemorrhage, epidural haematoma, epidural bleeding |
 | |
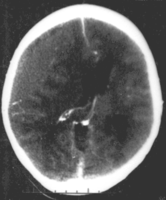
| Epidural hematoma as seen on a CT scan with overlying skull fracture. Note the biconvex shaped collection of blood. There is also bruising with bleeding on the opposite side of the brain. | |
| Specialty | Neurosurgery, Neurology |
| Symptoms | Headache, confusion, paralysis[1] |
| Usual onset | Rapid[2] |
| Causes | Head injury, bleeding disorder, blood vessel malformation[1] |
| Diagnostic method | Medical imaging (CT scan)[1] |
| Differential diagnosis | Subdural hematoma, subarachnoid hemorrhage, traumatic brain injury,[1] transient ischemic attack
burr hole)[1] |
Epidural hematoma is when bleeding occurs between the tough outer membrane covering the brain (dura mater) and the skull.[4] When this condition occurs in the spinal canal, it is known as a spinal epidural hematoma.[4]
There may be loss of consciousness following a head injury, a brief regaining of consciousness, and then loss of consciousness again.[2] Other symptoms may include headache, confusion, vomiting, and an inability to move parts of the body.[1] Complications may include seizures.[1]
The cause is typically head injury that results in a break of the temporal bone and bleeding from the middle meningeal artery.[4] Occasionally it can occur as a result of a bleeding disorder or blood vessel malformation.[1] Diagnosis is typically by a CT scan or MRI scan.[1]
Treatment is generally by urgent surgery in the form of a craniotomy or burr hole,[1] or (in the case of a spinal epidural hematoma) laminotomy with spinal decompression.
The condition occurs in one to four percent of head injuries.[1] Typically it occurs in young adults.[1] Males are more often affected than females.[1]
Signs and symptoms
Many people with epidural hematomas experience a
Other symptoms include severe headache; weakness of the extremities on the opposite side from the lesion due to compression of the crossed pyramid pathways; and vision loss, also on the opposite side, due to compression of the posterior cerebral artery. In rare cases, small hematomas may be asymptomatic.[3]
If not treated promptly, epidural hematomas can cause
]Causes

The most common cause of intracranial epidural hematoma is head injury, although spontaneous hemorrhages have been known to occur. Epidural hematomas occur in about 10% of traumatic brain injuries, mostly due to car accidents, assaults, or falls.[3] They are often caused by acceleration-deceleration trauma and transverse forces.[8][9]
Epidural hematoma commonly results from a blow to the side (temporal bone) of the head. The
A "heat hematoma" is an epidural hematoma caused by severe
Pathophysiology
The break of the temporal bone causes bleeding from the middle meningeal artery, [4] hence epidural bleeding is often rapid as arteries are high-pressure flow. In 10% of cases, however, it comes from veins and can progress more slowly.[10] A venous hematoma may be acute (occurring within a day of the injury and appearing as a swirling mass of blood without a clot), subacute (occurring in 2–4 days and appearing solid), or chronic (occurring in 7–20 days and appearing mixed or lucent).[3]
In adults, the temporal region accounts for 75% of cases. In children, however, they occur with similar frequency in the
Diagnosis
Diagnosis is typically by
Epidural hematomas usually appear convex in shape because their expansion stops at the skull's
Epidural hematomas may occur in combination with subdural hematomas, or either may occur alone.[10] CT scans reveal subdural or epidural hematomas in 20% of unconscious people.[15] In the hallmark of epidural hematoma, people may regain consciousness and appear completely normal during what is called a lucid interval, only to descend suddenly and rapidly into unconsciousness later. This lucid interval, which depends on the extent of the injury, is a key to diagnosing an epidural hematoma.[3]
-
 Nontraumatic epidural hematoma in a young woman. The grey area in the top right is organizing hematoma, causing midline shift and compression of the ventricle.
Nontraumatic epidural hematoma in a young woman. The grey area in the top right is organizing hematoma, causing midline shift and compression of the ventricle. -
 Non-contrast CT scan of a traumatic acute hematoma in the right fronto-temporal area.
Non-contrast CT scan of a traumatic acute hematoma in the right fronto-temporal area. -
 A diagram showing an epidural hematoma.
A diagram showing an epidural hematoma.



Treatment
Epidural hematoma is a
Medications may be given after surgery. They may include antiseizure medications and hyperosmotic agents to reduce brain swelling and intracranial pressure.[17]
It is extremely rare to not require surgery. If the volume of the epidural hematoma is less than 30 mL, the clot diameter less than 15 mm, a Glasgow Coma Score above 8, and no visible neurological symptoms, then it may be possible to treat it conservatively. A CT scan should be performed, and watchful waiting should be done, as the hematoma may suddenly expand.[3]
Prognosis
The prognosis is better if there was a lucid interval than if the person was comatose from the time of injury. Arterial epidural hematomas usually progress rapidly. However, venous epidural hematomas, caused by a dural sinus tear, are slower.[3]
Outcomes are worse if there is more than 50 mL of blood in the hematoma before surgery. Age, pupil abnormalities, and Glasgow Coma Scale score on arrival to the emergency department also influence the prognosis. In contrast to most forms of traumatic brain injury, people with epidural hematoma and a Glasgow Coma Score of 15 (the highest score, indicating the best prognosis) usually have a good outcome if they receive surgery quickly.[3]
Epidemiology
About 2 percent of head injuries and 15 percent of fatal head injuries involve an epidural hematoma. The condition is more common in teenagers and young adults than in older people, because the dura mater sticks more to the skull as a person ages, reducing the probability of a hematoma forming. Males are affected more than females.[3]
References
- ^ ISBN 9780323448383.
- ^ ISBN 9781605477817.
- ^ PMID 30085524, retrieved 2019-02-13
- ^ ISBN 9780199710041.
Epidural hemorrhage (epidural hematoma, extradural hemorrhage, or hematoma) Bleeding outside the outermost layer of the dural mater, which is thus stripped away from the inner table of the skull or spinal canal.
- ^ a b Epidural Hematoma in Emergency Medicine at Medscape. Author: Daniel D Price. Updated: Nov 3, 2010
- ^ Penn State University (2009). "Probing Question: What is 'Talk and Die' Syndrome?". www.psu.edu. Retrieved 2022-03-26.
- ^ Wagner AL. 2006. "Subdural Hematoma." Emedicine.com. Retrieved on February 6, 2007.
- ^ a b University of Vermont College of Medicine. "Neuropathology: Trauma to the CNS.", March 2005, Retrieved on February 6, 2007.
- ^ a b McCaffrey P. 2001. "The Neuroscience on the Web Series: CMSD 336 Neuropathologies of Language and Cognition." Archived 2007-04-06 at the Wayback Machine California State University, Chico. Retrieved on February 6, 2007.
- ^ a b c Shepherd S. 2004. "Head Trauma." Emedicine.com. Retrieved on February 6, 2007.
- ^ Graham DI and Gennareli TA. Chapter 5, "Pathology of Brain Damage After Head Injury" Cooper P and Golfinos G. 2000. Head Injury, 4th Ed. Morgan Hill, New York.
- PMID 11303253. Retrieved 2008-01-24.
- ^ PMID 23219455.
- ^ Singh J and Stock A. 2006. "Head Trauma." Emedicine.com. Retrieved on February 6, 2007.
- ^ Downie A. 2001. "Tutorial: CT in Head Trauma" Archived November 6, 2005, at the Wayback Machine. Retrieved on February 6, 2007.
- PMID 19535215.
- ^ a b "Epidural hematoma: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2019-02-12.