
Central neurocytoma
| Central neurocytoma | |
|---|---|
 | |
| Axial T1-weighted gadolinium-enhanced MRI image showing an enhancing mass with cystic changes consistent with central neurocytoma in the right lateral ventricle. | |
| Specialty | Oncology, neurosurgery |
Central neurocytoma (CNC) is an extremely rare, ordinarily benign intraventricular
Signs and symptoms
There is a wide range of symptoms that patients show. Symptoms can lie dormant, but come about due to
- Intracranial pressure
- Headache
- Papilledema
- Vomiting
- Light headedness
- Impaired mental activity
- Gait instability
In rare and extreme cases, more severe symptoms can be observed:
- Memory disturbance
- Dementia
- Hemiparesis[5]
- Seizures
- Hemorrhage
- Psychosis[6]
Pathology

On the macroscopic scale, CNC tumors are grayish in color, resembling the gray matter that comes with areas of
Tumor samples stained using
-
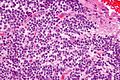 Very high mag.
Very high mag. -
 High mag.
High mag. -
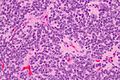 Very high mag.
Very high mag.



Diagnosis
This section is empty. You can help by adding to it. (December 2021) |
Treatment
The mainstay of treatment is surgical excision.[7] Two adjuvant therapeutic strategies are Stereotactic surgery (SRS) and fractionated convention radiotherapy (FCRT). Both are highly effective means of treatment.[8]
Surgery
Surgical excision of the central neurocytoma is the primary consensus among practicing physicians. The surgeons perform a craniotomy to remove the tumor. The ability to remove the tumor and to what extent it is removed is dependent upon the location of the tumor and surgeon experience and preference. The extent of the disease plays a large part in determining how effective the surgery will be. The main goal of a complete surgical resection, of the tumor, can also be hindered by the adherence of the tumor to adjoining structures or hemorrhages.[5] If there is a recurrence of the central neurocytoma, surgery is again the most notable treatment.
Radiotherapy
There is not much evidence supporting the claim that
Chemotherapy
Chemotherapy is typically limited to patients with recurrent central neurocytoma. The course of chemotherapy used for CNC is one of two platinum-based regimes. The two regimes are:
- Carboplatin + VP-16 + ifosfamide
- cisplatin + VP-16 + cyclophosphamide
Because chemotherapy is used in rare cases there is still information to be gathered as to the efficacy of chemotherapy to treat benign CNC. Therefore, recommendations must be viewed as limited and preliminary.[5]
Outcome and recurrence
The majority of patients can be expected to be cured of their disease and become long-term survivors of central neurocytoma. As with any other type of tumor, there is a chance for recurrence. The chance of recurrence is approximately 20%.
History
It was first described in 1982 by Hassoun.
Primary neuronal tumors occurring in the ventricular system were considered to be rare. Most cases described were of non-neuronal origin such as oligodendroglioma, ependymoma, meningioma, choroid plexus papilloma and giant cell. Neurocytomas were probably historically misdiagnosed as intraventricular oligondedronglioma or clear cell ependymoma prior to this. With its non-aggressive behavior the tumor has often been called "benign central neurocytoma". It is believed to occur in young adults from the neuronal cells of the septum pullicidum and the subependymal cells of the lateral ventricles. Most of the initial incidents reported in the lateral ventricle were benign. However, as more information was gathered the name benign central neurocytoma was started to be seen as a double misnomer because these tumors are not always benign nor centrally located. Many recent studies suggest that their location, biological potential and clinical behavior are observed be more variable than previously thought. Recent studies indicate their uncommon location, aggressive biological behavior and frequent recurrences following after surgical resection have generated significant interest in various treatment modalities and also in their terminology, lineage potential and molecular regulation.[13]
Epidemiology
CNC represent 0.1-0.5% of primary
References
- PMID 20692674.
- ^ S2CID 21557148.
- PMID 17618441.
- ^ PMID 23358787.
- ^ a b c d e Chamberlain, Marc C. Treatment of Central Neurocytoma. USC/Norris Cancer Center. Seattle Cancer Care Alliance. <https://www.seattlecca.org/client/Chamberlain_Treatment%20of%20Central%20Neurocytomas.pdf Archived 2014-03-24 at the Wayback Machine> Feb. 20 2014.
- PMID 15687074.
- S2CID 8320493.
- ^ S2CID 23101170.
- S2CID 12995192.
- ^ PMID 23205795.
- S2CID 6524741.
- S2CID 11054237.
- ^ S2CID 1245015.
- PMID 16163043.
- ^ S2CID 7854296.
- S2CID 19604295.