
Toxic epidermal necrolysis
| Toxic epidermal necrolysis | |
|---|---|
| Other names | pain medication[3] |
| Prognosis | Mortality 20–50%[2][3] |
| Frequency | 1–2 per million per year (together with SJS)[2] |
Toxic epidermal necrolysis (TEN), also known as Lyell's syndrome, is a type of severe
The most common cause is certain medications such as
Treatment typically takes place in
Signs and symptoms
Prodrome
TEN ultimately results in extensive skin involvement with redness, necrosis, and detachment of the top (epidermal) layer of the skin and mucosa. Before these severe findings develop, people often have a flu-like prodrome, with a cough, runny nose, fever, decreased appetite and malaise. A history of drug exposure exists on average 14 days (ranging from 1–4 weeks) prior to the onset of symptoms, but may result as early as 48 hours if it is a reexposure.[8]
Skin findings
Initial skin findings include red-purple, dusky, flat spots known as
-
 Toxic epidermal necrolysis on legs
Toxic epidermal necrolysis on legs -
 The emerging blisters on day 4 of an instance of TENs
The emerging blisters on day 4 of an instance of TENs -
 The back of a TENs patient on day 10, at the peak of the condition
The back of a TENs patient on day 10, at the peak of the condition



Mucosal findings
Nearly all people with TEN have oral, eye and genital involvement as well. Painful crusts and erosions may develop on any
Complications
Those who survive the acute phase of TEN often develop long-term complications affecting the skin and eyes. Skin manifestations can include scarring, eruptive
Cause
Drug reactions have been reported to cause 80–95% of TEN cases.[6]
The drugs most often implicated in TEN are:
- antibiotics
- nonsteroidal anti-inflammatory drugs
- allopurinol
- antimetabolites (methotrexate)
- antiretroviral drugs(nevirapine)
- corticosteroids
- anxiolytics (chlormezanone)
TEN has also been reported to result from infection with
HIV
HIV-positive individuals have 1000 times the risk of developing SJS/TEN compared to the general population. The reason for this increased risk is not clear.[7]
Genetics
Certain genetic factors are associated with increased risk of TEN. For example, certain HLA-types such as, HLA-B*1502,[14] HLA-A*3101,[15] HLA-B*5801,[16] and HLA‐B*57:01[17] have been seen to be linked with TEN development when exposed to specific drugs.
Pathogenesis
The immune system's role in the precise pathogenesis of TEN remains unclear. It appears that a certain type of immune cell (
Diagnosis
The diagnosis of TEN is based on both clinical and histologic findings. Early TEN can resemble non-specific drug reactions, so clinicians should maintain a high index of suspicion for TEN. The presence of oral, ocular, and/or genital mucositis is helpful diagnostically, as these findings are present in nearly all patients with TEN. The
Given the significant morbidity and mortality from TEN, as well as improvement in outcome from prompt treatment, there is significant interest in the discovery of serum biomarkers for early diagnosis of TEN. Serum granulysin and serum high-mobility group protein B1 (HMGB1) are among a few of the markers being investigated which have shown promise in early research.[7]
Histology
Definitive diagnosis of TEN often requires biopsy confirmation. Histologically, early TEN shows scattered necrotic keratinocytes. In more advanced TEN, full thickness epidermal necrosis is visualized, with a subepidermal split, and scant inflammatory infiltrate in the
-
 Confluent Epidermal Necrosis, low mag
Confluent Epidermal Necrosis, low mag -
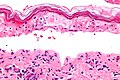 Confluent Epidermal Necrosis, high mag
Confluent Epidermal Necrosis, high mag


Differential diagnosis
- Staphylococcal scalded skin syndrome
- Drug-induced linear immunoglobulin A dermatosis
- Acute graft versus host disease
- Acute generalized exanthematous pustulosis
- Erythroderma
- Drug reaction with eosinophilia and systemic symptoms aka DRESS
- A generalized morbilliform eruption[18]
Treatment
The primary treatment of TEN is discontinuation of the causative factor(s), usually an offending drug, early referral and management in
Current literature does not convincingly support use of any adjuvant systemic therapy. Initial interest in
Numerous other adjuvant therapies have been tried in TEN including,
Prognosis
The mortality for toxic epidermal necrolysis is 25–30%.
Severity score
The "Severity of Illness Score for Toxic Epidermal Necrolysis" (SCORTEN) is a scoring system developed to assess the severity of TEN and predict mortality in patients with acute TEN.[23]
One point is given for each of the following factors:[12]
- age >40
- heart rate >120 beats/minute
- carrying diagnosis of cancer
- separation of epidermis on more than ten percent of body surface area (BSA) on day 1.
- Blood Urea Nitrogen >28 mg/dL
- Glucose >252 mg/dL (14 mmol/L)
- Bicarbonate <20mEq/L
Score
- 0–1: 3.2% mortality
- 2: 12.2% mortality
- 3: 35.3% mortality
- 4: 58.3% mortality
- ≥5: 90% mortality
Of note, this scoring system is most valuable when used on the first and third day of hospitalization, and it may underestimate mortality in patients with respiratory symptoms.[12]
References
- ISBN 978-1-4160-2999-1.
- ^ a b c d e f g h i j k l m n "Stevens-Johnson syndrome/toxic epidermal necrolysis". Genetics Home Reference. July 2015. Archived from the original on 27 April 2017. Retrieved 26 April 2017.
- ^ a b c d e f g h i j k l m n o "Orphanet: Toxic epidermal necrolysis". Orphanet. November 2008. Archived from the original on 27 April 2017. Retrieved 26 April 2017.
- ^ a b c d "Stevens-Johnson syndrome". GARD. Archived from the original on 28 August 2016. Retrieved 26 August 2016.
- PMID 28256714.
- ^ PMID 23866878.
- ^ PMID 23866879.
- PMID 1779014.
- PMID 7794310.
- PMID 20619392.
- ^ (PDF) from the original on 2019-12-03. Retrieved 2019-12-12.
- ^ PMID 22818644.
- ^ a b c Garra, GP (2007). "Toxic Epidermal Necrolysis Archived 2007-12-27 at the Wayback Machine". Emedicine.com. Retrieved on December 13, 2007.
- S2CID 45667604.
- PMID 21428769.
- S2CID 42286060.
- PMID 31314143.
- PMID 23866879.
- S2CID 25253929.
- S2CID 1477097.
- ^ from the original on 2018-06-25. Retrieved 2018-06-25.
- PMID 15967913.
- PMID 23866879.
External links
- 18-203e. at Merck Manual of Diagnosis and Therapy Home Edition
- DermNetNZ