
Palatine tonsil
| Palatine tonsil | |
|---|---|
Tonsillary branches of lesser palatine nerves | |
| Identifiers | |
| Latin | tonsilla palatina |
| MeSH | D014066 |
| TA98 | A05.2.01.011 |
| TA2 | 2853, 5181 |
| FMA | 9610 |
| Anatomical terminology] | |
Palatine tonsils, commonly called the tonsils and occasionally called the faucial tonsils,
Structure
The palatine tonsils are located in the
The palatine tonsil is one of the
Blood supply and innervation
The nerves supplying the palatine tonsils come from the maxillary division of the trigeminal nerve via the lesser palatine nerves, and from the tonsillar branches of the glossopharyngeal nerve. The glossopharyngeal nerve continues past the palatine tonsil and innervates the posterior 1/3 of the tongue to provide general and taste sensation.[7] This nerve is most likely to be damaged during a tonsillectomy, which leads to reduced or lost general sensation and taste sensation to the posterior third of the tongue.[8][9]
Blood supply is provided by tonsillar branches of five arteries: the
Tonsillar crypts
Palatine tonsils consist of approximately 15 crypts, which result in a large internal surface. The tonsils contain four lymphoid compartments that influence immune functions, namely the reticular crypt
Function
Local immunity
Tonsillar (relating to palatine tonsil) B cells can mature to produce all the five major
In addition to humoral immunity elicited by tonsillar and
Cytokine action
The cytokine network represents a very sophisticated and versatile regulatory system that is essential to the immune system for overcoming the various defense strategies of microorganisms. Through several studies, the
Clinical significance
The pathogenesis of infectious/inflammatory disease in the tonsils most likely has its basis in their anatomic location and their inherent function as organ of immunity, processing infectious material, and other antigens and then becoming, paradoxically, a focus of infection/inflammation. No single theory of pathogenesis has yet been accepted, however. Viral infection with secondary bacterial invasion may be one mechanism of the initiation of chronic disease,[12] but the effects of the environment, host factors, the widespread use of antibiotics, ecological considerations, and diet all may play a role.[13] A recent cross-sectional study revealed a high rate of prevalent virus infections in non-acutely ill patients undergoing routine tonsillectomy. However, none of the 27 detected viruses showed positive association to the tonsillar disease.[14]
In children, the tonsils are common sites of infections that may give rise to acute or chronic tonsillitis. However, it is still an open question whether tonsillar hypertrophy is also caused by a persistent infection. Tonsillectomy is one of the most common major operations performed on children. The indications for the operation have been complicated by the controversy over the benefits of removing a chronically infected tissue and the possible harm caused by eliminating an important immune inductive tissue.[15][16]
The information that is necessary to make a rational decision to resolve this controversy can be obtained by understanding the immunological potential of the normal palatine tonsils and comparing these functions with the changes that occur in the chronically diseased counterparts.
Acute tonsillitis
.jpg)
Tonsillitis is the inflammation of tonsils. Acute tonsillitis is the most common manifestation of tonsillar disease. It is associated with sore throat, fever and difficulty swallowing.[17] The tonsils may appear normal sized or enlarged but are usually erythematous. Often, but not always, exudates can be seen. Not all these signs and symptoms are present in every patient.
Recurrent tonsillitis
Recurrent infection has been variably defined as from four to seven episodes of acute tonsillitis in one year, five episodes for two consecutive years or three episodes per year for 3 consecutive years.[18][19]
Tonsillar hypertrophy
Tonsillar hypertrophy is the enlargement of the tonsils, but without the history of inflammation. Obstructive tonsillar hypertrophy is currently the most common reason for tonsillectomy.[15] These patients present with varying degrees of disturbed sleep which may include symptoms of loud snoring, irregular breathing, nocturnal choking and coughing, frequent awakenings, sleep apnea, dysphagia and/or daytime hypersomnolence. These may lead to behavioral/mood changes in patients and facilitate the need for a polysomnography in order to determine the degree to which these symptoms are disrupting their sleep.[20][21]
Additional images
-
 Lymphatic system
Lymphatic system -
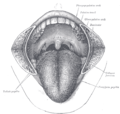 The mouth cavity. The cheeks have been slit transversely and the tongue pulled forward.
The mouth cavity. The cheeks have been slit transversely and the tongue pulled forward. -
 Throat after tonsillectomy
Throat after tonsillectomy -
 Anterior photograph of the oral cavity showing palatine tonsils (inflamed) anduvula.
Anterior photograph of the oral cavity showing palatine tonsils (inflamed) anduvula. -
 Open mouth with no visible palatine tonsils.
Open mouth with no visible palatine tonsils. -
 Palatine tonsil
Palatine tonsil






References
- ^ hednk-024—Embryo Images at University of North Carolina
- PMID 12928069.
- PMID 25051184.
- PMID 16386410.
- S2CID 28797083.
- ^ PMID 9745205.
- ^ PMID 34430822.
- S2CID 220943451.
- S2CID 25920988.
- PMID 3223268.
- PMID 22297210.
- PMID 27729119.
- PMID 22452646.
- PMID 32603480.
- ^ S2CID 198966664.
- PMID 28096515.
- S2CID 85565202.
- PMID 25407135.
- PMID 6700642.
- PMID 8280201.
- S2CID 34193798.
External links
- "Anatomy diagram: 05287.011-1". Roche Lexicon - illustrated navigator. Elsevier. Archived from the original on 2013-04-22.