
Paraganglioma
| Paraganglioma | |
|---|---|
| Other names | Chemodectoma, paraganglioma, carotid body tumour, glomus cell tumour |
 | |
| Micrograph of a carotid body tumor (a type of paraganglioma) | |
| Specialty | Oncology |
A paraganglioma is a rare
Signs and symptoms
Most paragangliomas are asymptomatic, present as a painless mass, or create symptoms such as hypertension, tachycardia, headache, and palpitations.
Genetics
About 75% of paragangliomas are sporadic; the remaining 25% are hereditary (and have an increased likelihood of being multiple and of developing at an earlier age). Mutations of the genes for the
Pathology


The paragangliomas appear grossly as sharply circumscribed polypoid masses and they have a firm to rubbery consistency. They are highly vascular tumors and may have a deep red color.[citation needed]
On microscopic inspection, the tumor cells are readily recognized. Individual tumor cells are polygonal to oval and are arranged in distinctive cell balls, called Zellballen.[8] These cell balls are separated by fibrovascular stroma and surrounded by sustentacular cells.[citation needed]
By light microscopy, the differential diagnosis includes related neuroendocrine tumors, such as
With
Sites of origin
About 85% of paragangliomas develop in the abdomen; only 12% develop in the chest and 3% in the head and neck region (the latter are the most likely to be symptomatic). While most are single, rare multiple cases occur (usually in a hereditary syndrome). [citation needed] Paragangliomas are described by their site of origin and are often given special names:
- Head and neck paraganglioma (HNPGL): There are various types of head and neck paraganglioma; they may have specialized names depending on the precise location.[9]
- Carotid paraganglioma (carotid body tumor): Is the most common of the head and neck paragangliomas. It usually presents as a painless neck mass, but larger tumors may cause cranial nerve palsies, usually of the vagus nerve and hypoglossal nerve.
- Glomus jugulare, also known as jugulotympanic paraganglioma: Both commonly present as a middle ear mass resulting in tinnitus (in 80%) and hearing loss (in 60%). The cranial nerves of the jugular foramen may be compressed, resulting swallowing difficulty, or ipsilateral weakness of the upper trapezius and sternocleiodomastoid muscles (from compression of the spinal accessory nerve). These patients present with a reddish bulge behind an intact ear drum. This condition is also known as the "Red drum". On application of pressure to the external ear canal with the help of a pneumatic ear speculum the mass could be seen to blanch. This sign is known as "Brown's sign". A deficient bony plate along the tympanic portion of the internal carotid artery (aberrant ICA) is a normal variant and can be mistaken with glomus jugulare.[10]
- Organ of Zuckerkandl: A collection of paraganglia near the bifurcation of the aorta, comprising a small mass of neural crest-derived chromaffin cells. Serves as a common origin of abdominal paragangliomas.
- Vagal paraganglioma: These are the least common of the head and neck paragangliomas. They usually present as a painless neck mass, but may result in dysphagia, hoarseness, or coughing with compression of the mass.
- Pulmonary paraganglioma: These occur in the lung and may be either single or multiple.[11]
- Other sites: Rare sites of involvement are the thoracic inlet, as well as the bladder in extremely rare cases.
Diagnosis
Classification
Paragangliomas originate from paraganglia in chromaffin-negative glomus cells derived from the embryonic neural crest, functioning as part of the sympathetic nervous system (a branch of the autonomic nervous system). These cells normally act as special chemoreceptors located along blood vessels, particularly in the carotid bodies (at the bifurcation of the common carotid artery in the neck) and in aortic bodies (near the aortic arch).[citation needed]
Accordingly, paragangliomas are categorised as originating from a neural cell line in the
Gallium-68 DOTATATE PET/CT imaging modality may be used to confirm the presence of a paraganglioma.[13]
Treatment
The main treatment modalities are
Additional images
-
 Micrograph of a carotid body tumor
Micrograph of a carotid body tumor -

-
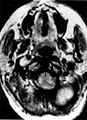 Ectopic functional paraganglioma (glomus jugulare) in a patient with VHL. T2 weighted MRI at the same location demonstrates a high signal mass consistent with a paraganglioma. Extra adrenal paragangliomas can be found in VHL (arrow).
Ectopic functional paraganglioma (glomus jugulare) in a patient with VHL. T2 weighted MRI at the same location demonstrates a high signal mass consistent with a paraganglioma. Extra adrenal paragangliomas can be found in VHL (arrow). -
 S100immunostainhighlighting the sustentacular cells in a paraganglioma
S100immunostainhighlighting the sustentacular cells in a paraganglioma -
 Digital subtraction arteriogram of carotid body tumor and jugular paraganglioma
Digital subtraction arteriogram of carotid body tumor and jugular paraganglioma


_in_a_patient_with_VHL.jpg)


See also
References
- PMID 24899893.
- ^ "Pheochromocytoma and Paraganglioma Treatment (PDQ®)–Patient Version - NCI". www.cancer.gov. December 23, 2011.
- S2CID 232159725.
- PMID 20071235.
- PMID 20154675.
- S2CID 205357831.
- PMID 29431636.
- PMID 17479683.
- .
- ^ Feky, Mostafa Mahmoud El. "Aberrant internal carotid artery | Radiology Case | Radiopaedia.org". radiopaedia.org. Retrieved 2017-05-02.
- PMID 16532231.
- PMID 10705811.
- PMID 27535829.
- PMID 14656575.
- PMID 15630855.
- ^ "Paragangliomas / Glomus Tumors of the Head and Neck". Stanford Medicine. Retrieved 16 March 2023.
External links
- Sampath Chandra Prasad; Carlo Terenzio Paties; Mattia Russel Pantalone; Renato Mariani-Costantini; Mario Sanna (July 2, 2019). "Carotid Body and Vagal Paragangliomas: Epidemiology, Genetics, Clinicopathological Features, Imaging, and Surgical Management". In Mariani-Costantini, R (ed.). Paraganglioma: A Multidisciplinary Approach. Codon Publications. PMID 31294944. Retrieved 16 March 2023.
- GeneReviews/NCBI/NIH/UW entry on Hereditary Paraganglioma-Pheochromocytoma Syndromes
| Authority control databases: National |
|---|