
Adrenocortical adenoma
| Adrenocortical Adenoma | |
|---|---|
| Other names | Adrenal cortical adenoma, adrenal adenoma |
Conn syndrome | |
| Specialty | Endocrinology, oncology |
An adrenocortical adenoma or adrenal adenoma is commonly described as a
Presentation
| Hypercortisolism | |
|---|---|
 | |
| Specialty | Endocrinology, oncology |
| Symptoms | Adrenal Lesion |
Adrenal adenomas are often categorized as endocrine-inactive tumors considering that majority of them are non-functioning and
Musculoskeletal
Cardiovascular
Endocrine and Metabolic
→More prevalent in males
→More prevalent in females
- Hyperandrogenism
- Irregular menstrual cycles
Neuropsychological
- Sleep disorders
- Depression
Skin
- Easy bruising
- Stretch marks
- Hirsutism
- Acne
Cause
| Adrenal Glands Zonations | |
|---|---|
 | |
| Specialty | Endocrinology, oncology |
| Adrenal Glands Zonations | |
|---|---|
 | |
| Specialty | Endocrinology, oncology |
Study of the reported cases indicate that most adrenocortical adenomas occur due to neoplastic proliferation of adrenal cortical cells within the three distinct layers of adrenal cortex. In humans, the adrenal cortex comprises three concentric zones including the zona glomerulosa, zona fasciculata, and zona reticularis that under normal conditions respond to body's physiological demands for steroid hormones. The adrenal cortex is considered a dynamic organ in which senescent cells are replaced by newly differentiated cells. This constant renewal facilitates organ remodeling which contributes to dynamic characteristics of the adrenal cortex.
Pathophysiology
If functional, adrenocortical adenomas can affect the normal activities of the adrenal cortex. Located within the adrenal glands are the three zones that are responsible for secretion of the three major classes of adrenal steroids. Hence, functional adrenocortical adenomas can induce over-secretion of adrenal steroids associated with pure or mixed endocrine syndromes, a condition commonly known as

Diagnosis
Due to their asymptomatic nature, most reported cases of adrenal adenomas have been discerned fortuitously through
Imaging Diagnostics
- Computed Tomography (CT scan)
- MRI)

Laboratory Tests
- CRH Stimulation Test
- High-dose dexamethasone suppression test
Gross Description
- Well-circumscribed lesion
- Size ≤ 5 cm
- Weight ≤ 50 grams
- often appear as golden-yellow color mass
(may have focal dark regions corresponding to
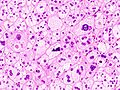
Histopathology

The microscopic histopathology analysis of the tissue samples obtained from the adrenal cortex of individuals presenting with adenoma-associated symptoms such as primary aldestronism (PA) indicates that adenoma cells are relatively larger with different cytoplasm, and increased variation in nuclear size. This indication is based on comparison between the healthy (normal) and affected (adenoma-associated) adrenal cortex tissue samples. [citation needed]
-
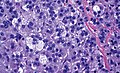 Adrenocortical adenoma with focal high grade nuclear atypia
Adrenocortical adenoma with focal high grade nuclear atypia -
 Adrenocortical adenoma with focal necrosis
Adrenocortical adenoma with focal necrosis -

-

-


_adrenocortical_adenoma.jpg)
_adrenocortical_adenoma.jpg)
_adrenocortical_adenoma.jpg)
Adrenocortical adenomas are most commonly distinguished from adrenocortical carcinomas (their malignant counterparts) by the Weiss system,[10] as follows:[11]
| Characteristic[11] | Score |
|---|---|
| High nuclear grade (enlarged, oval to lobated, with coarsely granular to hyperchromatic chromatin and easily discernible, prominent nucleoli)[12] | 1 |
| More mitoses than 5/50 high power fields | 1 |
| Atypical mitoses | 1 |
| Eosinophilic cytoplasm in >75% of tumor cells | 1 |
| Diffuse architecture of >33% of tumor | 1 |
| Necrosis | 1 |
| Venous invasion | 1 |
| Sinusoidal invasion (no smooth muscle in wall) | 1 |
| Capsular invasion | 1 |
Total score indicates:[11]
- 0-2: Adrenocortical adenoma
- 3: Undetermined
- 4-9: Adrenocortical carcinoma
Treatment
- Non-functioning cases of adrenocortical adenoma can be managed through long-term followups and monitoring.[citation needed]
- The treatment approach for the functioning cases of adrenocortical adenoma depends on the type of disorders they induce and their advancement. Surgical excision may be required if its presence is resulting in atrophy of the adrenal glands and the surrounding tissues.[citation needed]
In order to acquire better treatment strategies, it is important to further examine, study and discern the distinct molecular mechanisms involved in the formation of
A 2018 Cochrane Systematic review compared two different types of surgery: laparoscopic retroperotenial adrenalectomy and laporoscopic transperitoenal adrenelectomy in different types of adrenal tumors.[14] Laparoscopic retroperotenial adrenalectomy appeared to reduce late morbility, time to oral fluid or food intake and time to ambulation, when compared to laparoscopic transperitoenal adrenalectomy.[14] However there was uncertainty in these findings due to low-quality evidence, as well as inconclusive findings about effects of either surgery on all-cause mortality, early morbidity, socioeconomic effects, duration of surgery, operative blood loss, conversion to open surgery.[14]
Prognosis
- The long-term outlook for individuals diagnosed with non-functional adrenocortical adenoma is usually excellent.
- The long-term outlook for individuals diagnosed with functional adrenocortical adenoma is good with early diagnosis and treatment.
Epidemiology

- Prevalence: Female > Male
- More common in adults
- Relatively earlier onset in females (ages ≤ 20) than males (ages ≤ 30)
- Most common cause of ACTH-independent Cushing's syndrome
See also
- Hyperplasia
- Adrenal tumor
- Cushing's syndrome
- Conn's syndrome
- Hypercortisolism
- Hyperaldosteronism
- Hyperandrogenism
- Adrenal gland
- Adrenal paraganglioma
- Adrenal Pheochromocytoma
- Adrenal ganglioneuroma
References
- ^ "Definition: adrenocortical adenoma from Online Medical Dictionary".
- ^ PMID 30061126.
- PMID 31651844.
- PMID 31208392.
- PMID 30210105.
- PMID 23819074.
- PMID 25798129.
- PMID 28476230.
- ^ PMID 21455202.
- PMID 24102952.
- ^ ISSN 0857-1074.
- ^ Tito Fojo (26 December 2016). "Adrenocortical Cancer". Retrieved 2020-07-02.
- S2CID 40454423.
- ^ PMID 30595004.
- ^ Data and references for pie chart are located at file description page in Wikimedia Commons.
{kind=link}